


Saskatchewan "doctor" claims Premier lied about vaccines not reducing transmission
Or how a Saskatchewan doctor proves himself an idiot.

Edit: Excuse the error in the title that was sent out. I need an editor 😂
Someone sent me a news article featuring Alexander Wong, a guy who plays a doctor on television or something (at least it seems that way with all the air time he gets from Canadian media). He wrote a long-winded Twitter thread explaining why Scott Moe’s letter upset him. In the thread, he made two claims and posted three studies to back up his argument.
Let’s take a look.
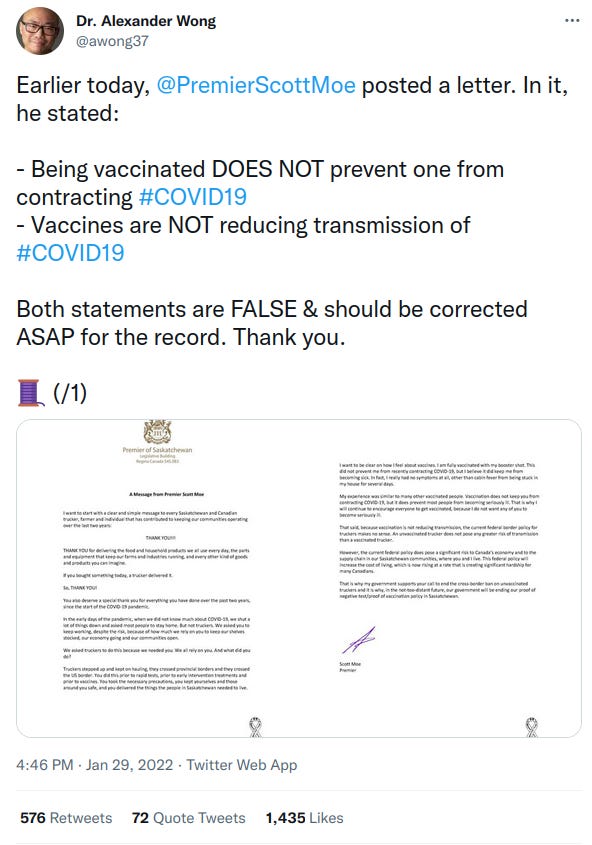
So his two claims are
Vaccination PREVENTS one from contracting COVID; and,
Vaccination REDUCES transmission.
If claim (1) were true, then claim (2) would necessarily be true. He could have won the argument quickly if claim (1) was not a blatant lie. Preventing someone from contracting COVID implies that the vaccines are sterilizing. They are simply not.
Here is an excellent article by a pro-vaccine individual on why the cake is a lie.
But we also know the vaccines do not have sterilizing immunity because we continue to observe, in the real world, huge proportions of the vaccinated being infected. This fact has not been contested, as far as I am aware, by even the most ardently pro-vaccine individuals, aside from Wong. I personally think Wong even making that claim, with absolutely no evidence to support it and even though all evidence points against it, devalues any further claim he makes, but let’s continue just for fun…
Claim (2) is what we are actually debating. There are three possible scenarios: the vaccines increase transmission, do nothing to prevent transmission, or reduce transmission. Most observational data in Canada, at the very least since omicron came on the scene, suggest that the vaccines increase transmission. Not only does Alexander Wong argue that what we are seeing in the data is not true, but he argues that the vaccines are still quite effective. His argument would be more powerful if he fought one dragon at a time and explained why the observational data is incorrect, but instead he lets’ studies speak for him. He presents the studies uncritically expecting people to accept the results uncritically.
But let’s get critical.

Of course, this type of study is my old nemesis, a test-negative case-control design. Remember the most important assumption of this type of design requires the same type of people going to the hospital for the same type of reason with the same type of test.
This is taken directly from the study he cites:
Study setting
KPSC is an integrated health care system that provides care to more than 4.6 million socio-demographically diverse health plan members at 15 hospitals and associated medical offices across Southern California. Comprehensive electronic health records (EHRs) used for this study included information on demographics, immunizations, diagnoses, laboratory tests, procedures and pharmacy records. KPSC began administering mRNA-1273 on 12/18/2020. Outside COVID-19 vaccinations were imported into members’ EHRs daily from external sources, including the California Immunization Registry, Care Everywhere (system on the Epic EHR platform that allows health care systems to exchange members’ medical information), claims (eg, retail pharmacies) and self-report by members (with valid documentation).
Laboratory methods
Molecular diagnostic testing for SARS-CoV-2 is available to members who request it for any reason, before procedures and hospital admissions, with and without symptoms. Specimens were primarily collected using nasopharyngeal/oropharyngeal swabs (for symptomatic individuals) or saliva (for asymptomatic individuals).
The study, like most of its kind, does not even attempt to validate or address the assumption. The supplementary index is not very helpful as we do not have population characteristics, but 57% of the total cases including with both delta and omicron were in the vaccinated. 15.1% of positive tests were saliva based (asymptomatic, I suppose?) with the saliva based tests more likely to test negative than the nasal tests. There is also a mishmash of people that would test for different reasons that really cannot be controlled for in any meaningful way.
I rate this study as poorly designed and useless in the face of the observational data we have before us. I hope he didn’t lead with his best evidence.

Annnnnd… the second study is also a test-negative case-control design. Do people recall my previous article where I told you to be ready for these because we will be seeing a lot of them? They are the go-to study design for vaccine enthusiasts trying to obfuscate the observational data. How does the assumption do?
Data sources
We linked provincial SARS-CoV-2 laboratory testing, reportable disease, COVID-19 vaccination, and health administrative databases using unique encoded identifiers and analyzed them at ICES, a not-for-profit provincial research institute
Nope. Treating the entire province as if they are similar and testing for similar reasons means this study failed before it started. Again, you cannot control for the differences in testing behavior here.
Even more ridiculously, we know the vaccination breakdown of the entire province (unlike the last study that only used a few KP hospitals). So how many cases were in each cohort?
Get ready for it.
There were 797 cases in the unvaccinated, 13852 cases in the double vaccinated, and at least 2276 in the boosted (there was one category that was <5).
Sorry, but 95.3% of all cases in the vaccinated and still effective at reducing transmission, Alex? But maybe you saved the best for last…

Nope. Test-negative case-control design.
You would think for such a highly effective vaccine you could show it is effective in more than one way. At least this one only included symptomatic people that tested, so maybe he did save the best for last?
Again, here is where I see the study violating the required assumption in a large way.
Data from the ICATT platform—a Department of Health and Human Services (HHS) partnership facilitating no-cost, drive-through SARS-CoV-2 testing at pharmacies across all 50 states, the District of Columbia, and Puerto Rico—were analyzed. Testing sites were selected by HHS to prioritize access in racially and ethnically diverse communities and areas with moderate-to-high social vulnerability.
Test-negative designs are extremely limited use study designs, and, honestly, probably require a clinical setting to even be useful for vaccines. I don’t see how this is the same people testing for the same reasons. No-cost drive-thru testing sites in prioritized for access to racially and ethnically diverse communities, really?
It is interesting that a full 74% of all positive cases were in the fully vaccinated or boosted in a country where only 64% of the population has been fully vaccinated (as of today and less during the study period). Of course, partially vaccinated are excluded, so that means you would expect less than 72.7% of cases to be in the vaccinated… and significantly less for a highly effective vaccine. Except vaccination rates are lower in racially and ethnically diverse communities in the US.
I can only come to one conclusion from the data presented: Alex Wong is an idiot.
...aaannnd Justy Trudope himself, allegedly triple-jabbed, just tested POSITIVE, so....🤔
There's another possible conclusion, which substitutes mendacity for idiocy.