

The Church of COVID and the "New Normal".
The Church of COVID and the "New Normal".
Oh, the Hysteria!

One of my friends is a member of the Church of COVID. He doesn’t preach the gospel or anything—he tends to shy away from any mention of vaccine mandates. But he gets his boosters on a schedule and has been legitimately scared of the virus since the beginning.
Why?
Simply put, he reads Twitter threads like this one from Stephanie Tait.

I will not post the whole Twitter thread—honestly, most of it is simply fear mongering. She, like my friend, appears to have bought into two years of gaslighting and has used her platform to spread a message using numbers that she doesn’t quite understand. The example below is quite illustrative.
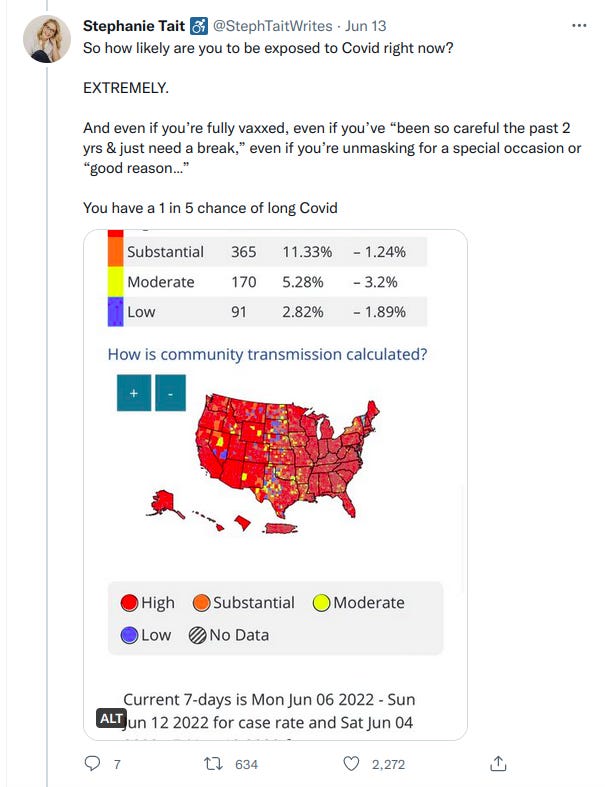
Stephanie is referencing data from here, which, of course, comes directly from the heart of the Church itself — the CDC.
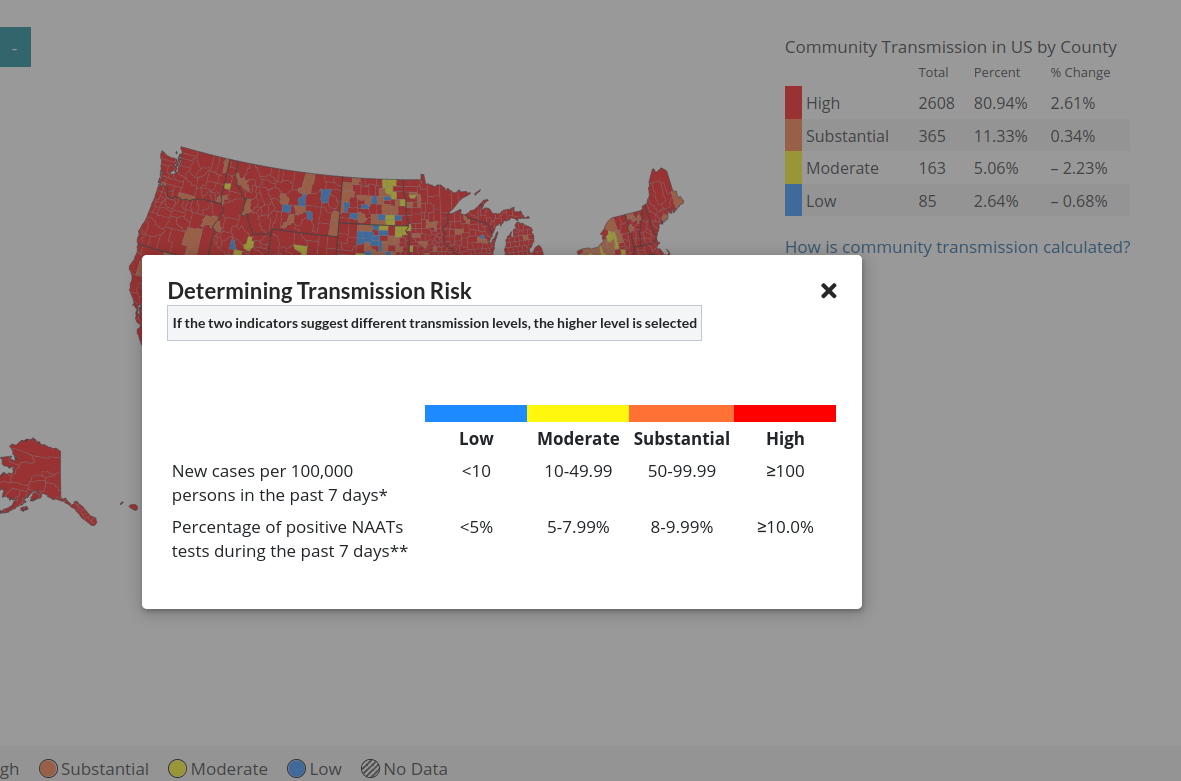
I doubt she ever clicked on the link explaining how community transmission is calculated. No, members of the Church usually ignore small details like methodology and scale. If she had gone a step further, though, she would have found that in order to be in the ‘high’ category, a county only needs greater than 100 cases per 100,000 population. Or 1 in 1000 for those counting. Presumably, most sick people are not out and about in the community at all, choosing to stay at home or otherwise congregating in places where community spread may be higher, such as clinics.
As far as a metric of determining transmission risk, the map says very little. To extrapolate and say one is “EXTREMELY” likely to get the virus based on that map is to say that you lack the ability to think critically about complex subjects, Stephanie.
As an example, where I live would be in the “high” transmission risk category, yet I spent two days last week at a conference with several hundred people put into a room with no social distancing including a buffet lunch thereby exposing myself to a much higher risk than one would face in the community on a given day. Did I get sick? No. Was it a “super spreader” event? No. People who were sick simply chose to stay home and rest. That does not fit the definition of extremely risky to me.
Inexact, subjective terms aside, I wanted to specifically discuss the numbers that Stephanie did provide in the first post in her thread.
Again, I question whether she went a step beyond the tweet with a link to a Forbes article that she is referencing and I am nearly certain she did not click the link to the ‘studies’ within the article. But I am absolutely certain that she did not understand the source material even if she made it that far.
There are three ‘studies’ that the Forbes article mentions which reference rates.
The first study is actually an old Office of National Statistics study out of the United Kingdom. Forbes uses this for their “low" estimate of how many people have long-COVID, 10% (the study itself was actually a range with 13.7% being the number the authors landed on).
The second “study” out of California uses outpatient data (ie., clinic setting) to estimate up to 30% of people have long-COVID (actually 27%).
The third “study” is survey data from social media groups of people that identify as having long-COVID.
If you had told me you could pick three sets of less believable data, I would not have believed you.
The ONS Study
The ONS study claims that 13.7% of those who tested positive for COVID experienced symptoms longer than 12 weeks. They match this up against a supposed control group of people that were “unlikely” to have been infected with COVID, 1.7% of which had symptoms that lasted longer than 12 weeks. Yikes. Looks like Stephanie is right! Case closed!
But wait just a minute.
A few months after that study was published, the authors updated the methodology leading to strikingly different results (which has the added bonus of saving me a lot of time criticizing the methodology). In the first method the authors used, 5% of those with COVID reported symptoms 12 to 16 weeks after infection compared to 3.4% in the control group.
There are additional confounding variables that the authors did not consider, which are hidden assumptions. Many of the symptoms are non-specific and occurred during a time when long-COVID talk was all the rage. There is an unknown psychosomatic factor here especially when talking about symptoms like “fatigue”.
Furthermore, participants in the survey are randomly selected (as far as I know); however, they are not randomly selected into the COVID and the control groups. This is extremely important for two reasons.
The way that participants treated COVID may have had detrimental effects on long-term health. Were ventilators used? Drugs? Et cetera.
The factors that contributed to these individuals being infected with COVID in the first place may very well be the reason that they have a higher prevalence of symptoms. Are these individuals more unhealthy in general? Overweight? Immuno-compromised? We simply do not know. The survey only matched participants by age, sex, and an extremely general question on whether they had an underlying health condition expected to last 12 months or more.
The authors also use a second method similar to the method in the original article correcting for one of their mistakes. Using the updated method, 3% in the COVID group had “continuous” symptoms and 0.5% of the control group did. Not having continuous symptoms means participants went two surveys without having any symptoms. Unfortunately, their methodology is still flawed as individuals in the control group, by proxy of not having COVID at week 0, only need to answer the survey one more time without symptoms to drop from the potential group with continuous symptoms. Whereas, the COVID group need to respond two more times without symptoms. This is a huge flaw and a more “fair” method would be for the control group to need to go three weeks without symptoms compared to the COVID groups two. Finally, the two factors I identified in the first method still apply to this method, making the actual outcomes even less clear.
The California Study
The second study that claims 27% of infected people get long-COVID belongs in the trash bin. Honestly, very little needs to be said about this study beyond the fact that there is no baseline/control group. The authors use a plethora of random symptoms, grasping at straws and including things as innocuous as heartburn, in order to argue that 27% of people who are infected with COVID get long-COVID. Except, all they prove is that 27% of people in a non-random sample over an unspecified period of time will have a random health condition.
Interestingly, they post a graph in the appendix that references a control group, but that is the only reference in the entire study. Yikes.
The Social Media Survey
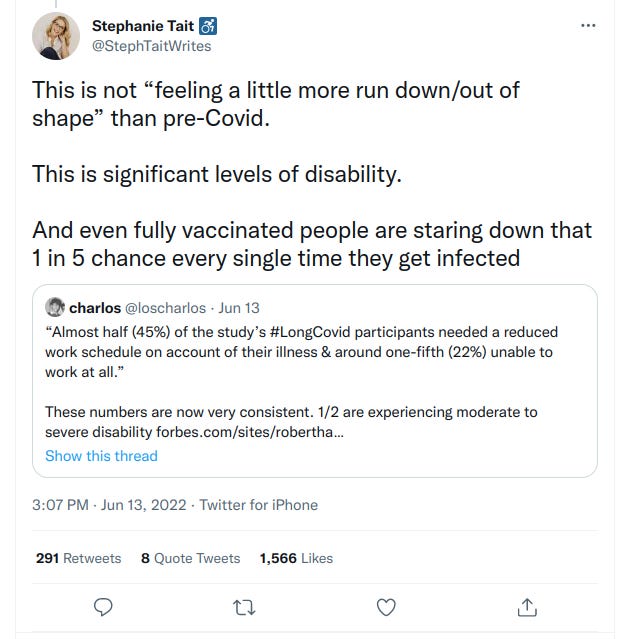
Finally, the social media survey is what Stephanie uses to justify how “horrible” so-called long-COVID truly is!
We conducted an online survey of people with suspected and confirmed COVID-19, distributed via COVID-19 support groups (e.g. Body Politic, Long COVID Support Group, Long Haul COVID Fighters) and social media (e.g. Twitter, Facebook).
The question is why did the authors waste their time and why did Lancet publish this garbage? It would be like taking a poll outside of Alcoholics Anonymous inquiring how many people like to drink. Well, at least if Alcoholics Anonymous was full of psyche patients who may or may not have drank in their life.
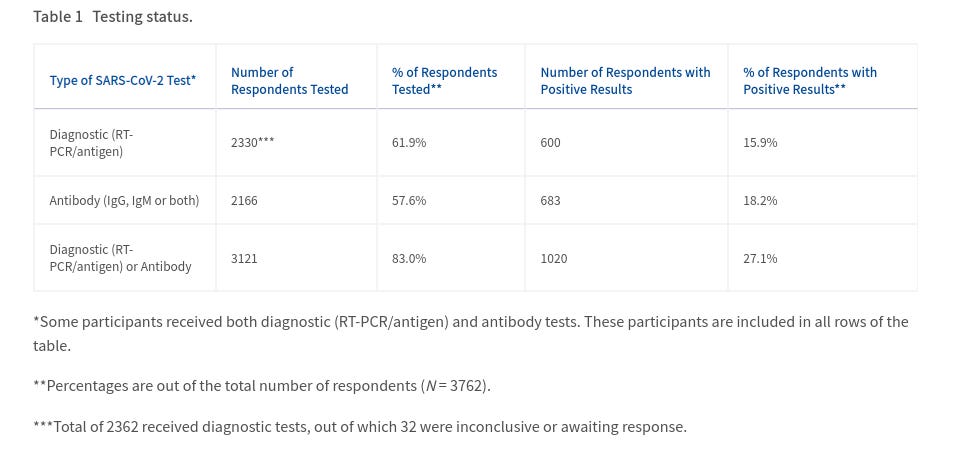
In fact, only 27% of the people surveyed in these groups tested positive for COVID. Let’s recall that Stephanie was citing a tweet that claimed 45.2% had a reduced work schedule and 22.3% were not working. That 45.2% is from the total survey population of 3762 respondents. Or about 700 more than even tested positive for COVID.
The inclusion criteria is equally insane. It is limited to people whose symptoms lasted more than 28 days and had symptom onset between December 2019 and May 2020. Hypochondriacs during peak hysteria.
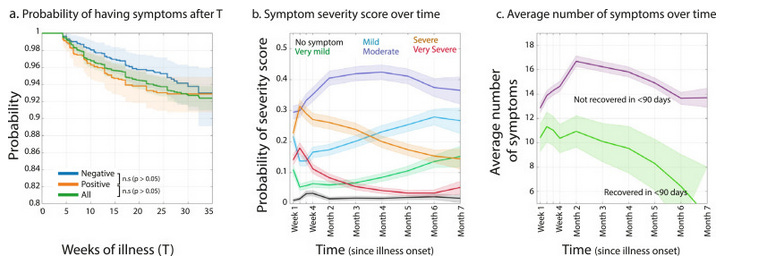
In fact, the probability of someone having symptoms was higher in the people that tested negative for COVID!
Yikes! I don’t think this “study” deserves any more attention than that.
Conclusion
Stephanie Tait is hysterical. She bought in hard to the Church teachings, or perhaps she just wants to make a few dollars more selling her books. But people legitimately believe her, people like my friend who gets his boosters on a schedule.
Well, after his last booster, he has been having health troubles. He believes it is anxiety but says ever since he got the shot he feels like he is going to have a heart attack. Whether it is an adverse event from the booster or anxiety from reading Twitter threads like Stephanie’s, one thing is clear, the Church of COVID is a destroyer, looking for martyrs, and he is the latest one.
Edit: I should note none of these studies would have improved the strength of her argument even if they agreed with her claim as they were all done in periods long before omicron.
One of my best friends is now a martyr, he believed the Church and paid the ultimate price via a heart issue.
Beyond MASKS FOREVER, I qonder what is their idea of the future? Her Twitter threads have some talks of therapeutics, but I can't find any drugs/vitamin names, making me think the Covid Church is all in on Paxlovid and chicken soup.
Sad times ahead for all of those people living in abject fear of living.
It really is a mental issue, very hard to understand but I know people like this. The infuriating thing is that government, media, and health "care" all conspired to create this mental illness.