


Lethal Injection
Myocarditis, pericarditis, and cardiac arrhythmia in the U.K.

“Before they give you a lethal injection, they swab your arm with alcohol. It's true.”
George Carlin
Incidentally, the symbolic process of sterilization becomes part and parcel of the punishment. The strangest takeaway from the last couple years has been the punishment being alleviated only by the symbolic process of sterilization. The vaccines, in fact, are non-sterilizing. They do not stop the virus in its tracks as initially promised, but seem to use the bodies of the vaccinated as vessels to move through society unimpeded.
Even more strangely, a significant portion of society has been captured by the idea that vaccination will provide clemency from the government’s heavy hand. In a sense, the non-believers must be punished in order to bring about a new golden age of occasional periods of hope in between routine lock-downs. Such a new normal makes me wonder if there ever were a country with perfect vaccination uptake, who would the vaccinated scapegoat? The unvaccinated in other country? The unboosted? Certainly neither themselves nor their slave-masters.
In any case, the reason we will not see perfect vaccination is not because the vaccine has a three-month half-life, though that would be an excellent reason, but rather because there are a myriad of side-effects and unknowns associated with the injections. To name just a few: blood clots, autoimmune disorders, neurological problems, damage to the immune system, and, ah yes, heart issues.
The latter group of adverse events is, perhaps, the most well-documented or at least well-publicized of the them all (though, I would argue, not anywhere near the most damning). But while all except the most dishonest actors have acknowledged the vaccines are causing heart issues, the data still barely trickles into the mainstream. Often, when some truths do arise, the conclusions are filled with “ifs and buts”. For example, this article out of Nature is the quintessential pro-vaccine, adverse event acknowledgement.
The article does not, of course, preclude that the presence of adverse events, but rather tries to contextualize them alongside Sars-CoV-2. I do not have a problem with doing so, but I do have a problem with the limited viewpoint of the authors on the true risk of getting the virus versus getting the vaccine. For one, whenever we talk about the number needed for an event to occur, it should be noted that not everyone gets the virus, but everyone gets the vaccine. And getting the vaccine does not preclude one from getting the virus as well. Furthermore, the vaccine is not a single event, but rather, multiple and potentially endless events.
At the very least, given the short half-life of the vaccination, three vaccines per year should be a minimum consideration. Whereas, the risk of the virus can never be a certainty and, at the very least, may only occur once every few years to any given individual from a probabilistic standpoint. Depending on how persistent natural immunity is in the long-term, every few years may be an overstatement.
Before discussing the study, I want to point my subscribers in the direction of this excellent analysis of the study method used by the authors of the paper by Bartram at Batram’s Folly’s. Please give his article a close reading and some likes as it truly is an excellent analysis of the problematic use of this particular study design.
So, from my perspective, there are many eye-opening findings in this study. First of all, given what we know about natural immunity, the fact that many people had the virus in the pre-vaccination period and yet still got vaccinated is criminal. If the logic is that the virus also causes heart complications, then why would people expose themselves to further complications after acquiring a much more robust form of immunity to the virus? This could have been forgiven at the beginning of the vaccination rollout before it was evidently clear that the vaccines offered at best short-term protection; however, public health experts have known for a long time about this particular limit to the vaccine. Yet, these same “experts” still, to this day, fail to recognize natural immunity. As I said, criminal.
Keeping Bartram’s post in mind (ie., the IRR for the vaccinated are likely underestimated), we should consider the fact that the cases in the Sars-CoV-2 population are almost certainly overestimated, and likely be a lot.
The reason for this is the authors of this paper are using a data set to match individuals in the population that relies on testing. In short, we are not seeing cases that are not subject to testing. Corollary, those that go to the hospital for any reason are likely to get tested for the virus, so people with myocarditis are going to the hospital and getting tested, rather than getting the virus and then subsequently getting myocarditis.
Generally, it takes a few days for symptoms to appear for the virus, so one would expect if the virus was the main driver here, the incidence rate be higher in the days following the test, rather than on day 0. Instead, the incidence rates are by far the highest on day 0 when people are getting diagnosed with heart issues. This means that the virus may be incidental in many of these cases. Perhaps, a better metric, if the study is already using a pre-vaccine period, there should be a similar post-positive test period. But I digress. Take a look at the screenshot below to see what I mean.
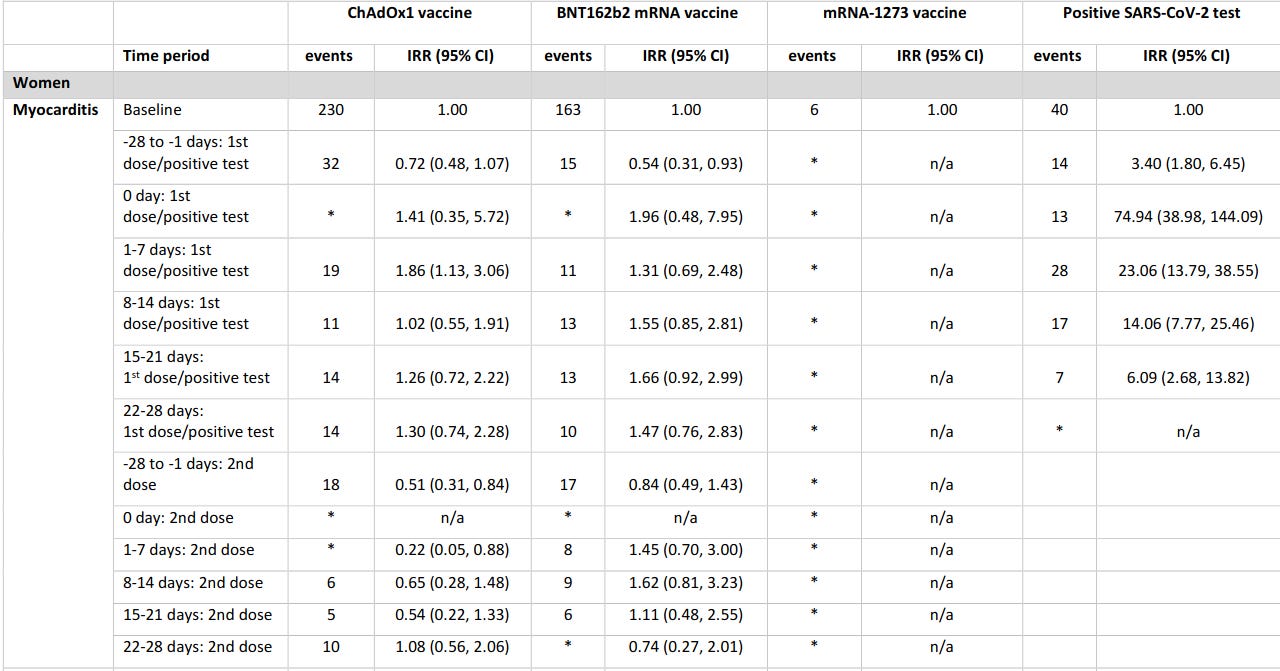
That said, to give the devil its due, there does appear to be a (albeit overestimated) effect of heart issues from catching the virus. However. as stated, this effect is way out of proportion just due to the limitations inherent in the data.
Another interesting point to note is the risk of heart issues seems to rise with subsequent shots in relation to the Moderna mRNA-1273 vaccine. This does not bode well for booster recipients. Also note, in the screenshot below, what I mentioned earlier. Everyone gets the shot, not everyone gets the virus. Furthermore, the shots are cumulative. As in, people are not exposed to the risk once, so the shots really need to be looked at together. The authors did not do this; those who had heart issues after the first shot were subsequently dropped out of the data set.
I see why the authors took that action; theoretically, those with complications from the first dose would be less likely to get the second dose, creating a downward bias on the data set and an upward bias on IRR. But it would be interesting to see the effect on individuals that had an adverse event on the first dose and still got the second dose.

Again, from the above, we the risk increases substantially for the younger population (who would be at the least risk from the virus in the first place). Here is how I would look at it if I was about to get vaccinated.
If I had a prior infection, the risks from both doses are all downside risk.
If I was Sars-CoV-2 naive, I would consider the risks from both doses and the reduced risk of getting an infection if I got vaccinated and I would consider the fact that there is an increased risk of getting an infection directly after getting vaccinated (which should be baked into the former point, but is usually overlooked by policy makers). Then, I would consider the risks of all subsequent doses.
You see, of course, how the table misses most of that nuance? That’s fine. Doctors these days miss most of it in general.
The death data is also interesting. I would question the Moderna mRNA-1273 data as it just appears to be missing (0 deaths for cardiac arrhythmia? Hmm). But the point that stands out to me is the mean age of death. With the vaccines, the mean age of death is much lower for myocarditis than for the positive test data, and deaths due to pericarditis are lower for the Astrazeneca ChAdOx1n vaccine than for the Pfizer BNT162b-2 vaccine, but that could be due to a small data set. The age matters because if the virus only kills the very old but the vaccine is killing the very young, even if the virus is better at killing the very old, giving the vaccine to the very young is a bad idea.
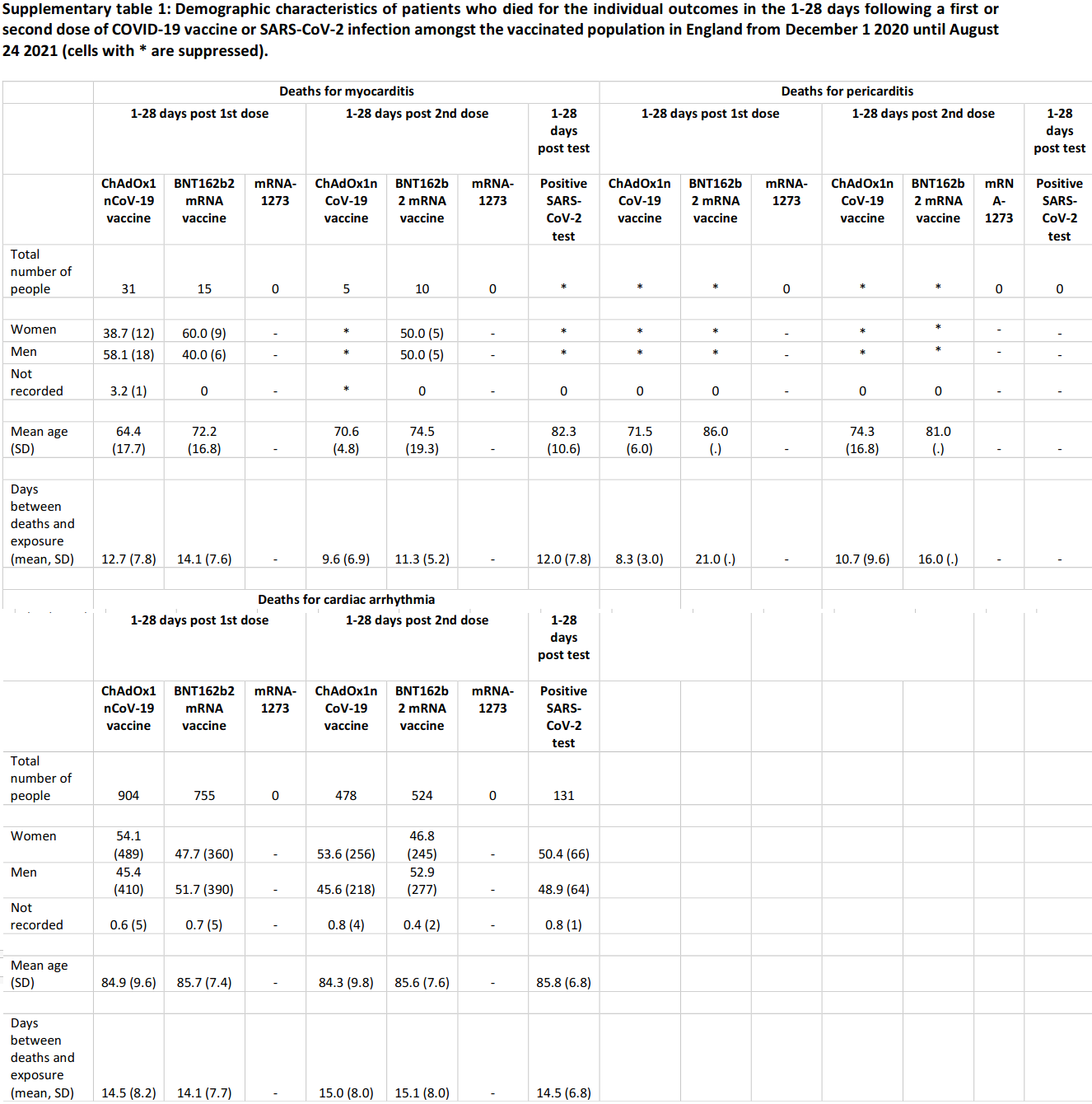
More interestingly though, it makes me wonder why the study leaves out a lot of deaths.
The main paper notes there were 114 deaths (23 with a positive test), yet most of those deaths are not in this section. Why?
31 deaths were due to pericarditis, 6 with a positive test. Again, omitted.
7,795 deaths with cardiac arrhythmia, 1108 with a positive test. And yet again, many omitted.
It is, indeed, strange that the supplementary material does not match the material in the paper. Maybe I am missing a very good reason for that, but I cannot think of one (. I was also disappointed the paper did not include tachycardia into the analysis as, though under-powered, the Pfizer vaccine trial data suggested this may be a statistically significant adverse event if the trial had been powered to find good safety information.
Another couple of takeaways, the authors due note that myocarditis in particular after vaccination is likely underestimated as, traditionally, the condition is underestimated.
Either way, it is interesting to, at least, see some large scale data on the issue even if the study method was, as Bartram noted, used inappropriately. Essentially, a lot of people who were previously infected were exposed to a lot of unnecessary risks, and a lot of those without an infection were exposed to extra forms of risk with little care and consideration. Now, if the authors could fix their study design and look at the age-groups we are concerned about rather than grouping people inappropriately, that would be great.

Alex Berenson had an interesting post on how they use (or don't) medical billing codes to obscure the cause of death, as there is no code for "vaccine" being the "cause" of death. I can recall reading a number of obituaries over the past year of people that died "after a short illness", which, in the cases I'm familiar with, seems to be a euphemism for "shortly after getting vaccinated". Most of these people were pretty old. Which begs the question: how can they keep saying that vaccines are "effective" for the "most vulnerable" (i.e. the sick and elderly)? That age cohort seems to me to be dying in droves from both COVID and/or the vaccines. But its all obscured because "old people die all the time". But that doesn't explain the skyrocketing life insurance claims paid for 25-65 yo that are demonstrably NOT from COVID... All part of the Plandemic, I guess...