


Pre-print study estimates VE against omicron will be extremely low.

The study out of the University of California, Santa Cruz has an interesting structure, if nothing else.
The researchers use an assumption of a 40-fold reduction in neutralizing antibody titers against omicron. I have only seen the South African study claiming a 40-fold reduction in neutralizing antibody titers, which had more researchers than research participants, so I am not sure how strong this assumption will turn out to be. That said, the short interval where the vaccine is effective seems to rely heavily on antibody titers unlike natural immunity, say, which has a wider range of tools to combat the virus.
Then, the researchers estimate omicron-VE in three discrete states: recently (fully) vaccinated, waned, and boosted. Obviously, using discrete states is not realistic, but I will forgive the authors here for the sake of modelling. However, it should be noted that using discrete states will inevitably make VE appear artificially high.
Why?
Well, consider the states that they selected. Recently (fully) vaccinated individuals had to suffer through a relatively long period of negative VE (initial vaccination) and may have yet to reach a break-even point1, thus, true VE for the entire vaccination period will be much lower than starting part way through the game.
Consider, for fun, the analogy of a football game. Here are two graphs with points measured from the same game. Figure 1 measures points scored from about mid-way through the third quarter onward, and Figure 2 measures points scored during the entire game.
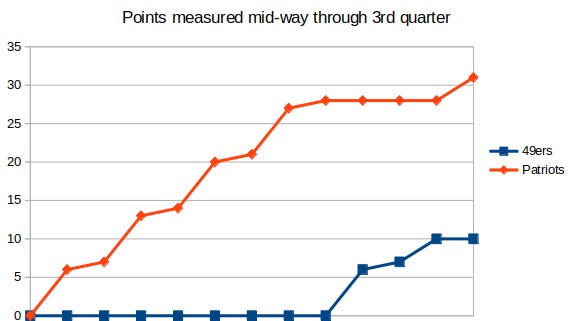
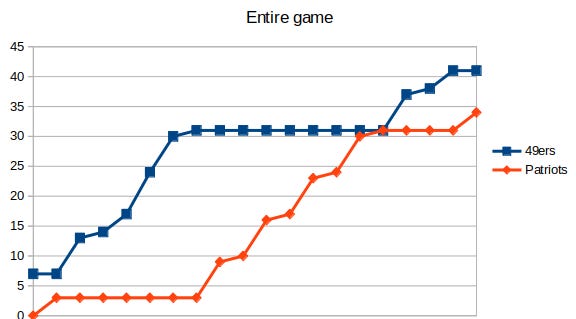
I am sure the Patriots would have loved to start counting midway through the 3rd quarter as two distinctly different pictures are painted.
But back to the study — the authors used a living review of the literature to estimate the VE for each of the various variants, and used these to inform their estimates for omicron. The researchers considered five endpoints: all infections, documented infections, hospitalizations, symptomatic disease, and transmission.
What did they find?

Well, as you can see, neither vaccine, according to their model, is useful in any way in reducing transmission. Those with waning antibodies, which is most of the population by now, get barely any protection against infections or symptomatic disease. Indeed, even those recently vaccinated or booster have little in the way of VE.
The study does claim that despite their assumption of a 40-fold reduction in antibodies, the vaccinated will still be highly protected against hospitalization despite the fact that the vaccines do little else (at least in terms of being mildly useful) besides producing antibodies. But that may be due to poor data access on the authors part rather than their own bias.
In any case, if the model used in this study is even remotely close to the truth, then we should all pay close to attention over the coming months. The amount of doublespeak by politicians trying to justify lock-downs could reach a whole new level, and our vaccine enthusiasts will likely get another 3-doses of New Pfizer (if New Coke was laced with trace amounts of poison) in their future.
The point where the cumulative virus-risk of the vaccinated individual is equal to that of the cumulative virus-risk of the unvaccinated individual. For one of the more recent clinical trials for Covaxin, this did not occur until approximately 80 days after initial vaccination. But the cumulative risk will change based on local wave dynamics.
And important to note about COVAXIN trial-- if it contributed or caused the worst outbreak on earth of Covid yet, then their "restored vaccine effectiveness" is equivalent to measuring burn marks from initial shockwave pilots dropping a nuke faced vs those who were incinerated.
Covaxin had within the first 28 days 27 cases and the placebo had 15. This is 73% increase in cases within 28 days before second dose. That's more than their overall efficacy.
This one? https://www.medrxiv.org/content/10.1101/2021.12.10.21267594v1.full.pdf